Akinniyi A Aje ![]() ,
Koreayode A Davies
,
Koreayode A Davies
For correspondence:- Akinniyi Aje Email: aje123@gmail.com Tel:+2348035684484
Received: 12 March 2015 Accepted: 19 October 2016 Published: 25 February 2017
Citation: Aje AA, Davies KA. Pharmaceutical care and the use of routine diagnostic tools by community pharmacists in Ibadan, Nigeria. Trop J Pharm Res 2017; 16(2):471-475 doi: 10.4314/tjpr.v16i2.28
© 2017 The authors.
This is an Open Access article that uses a funding model which does not charge readers or their institutions for access and distributed under the terms of the Creative Commons Attribution License (http://creativecommons.org/licenses/by/4.0) and the Budapest Open Access Initiative (http://www.budapestopenaccessinitiative.org/read), which permit unrestricted use, distribution, and reproduction in any medium, provided the original work is properly credited..
Purpose: To evaluate the use of routine diagnostic tools among community pharmacists in Ibadan, Nigeria.
Methods: This is a cross-sectional study with pre-tested questionnaire administered to 94 pharmacists in community pharmacies in Ibadan, southwestern Nigeria. Descriptive statistics was used to summarise data and categorical variables were compared with Chi-square at a significance level of p < 0.05.
Results: With a response rate of 94.7 %, the study showed that 78 (87.6 %) of the respondents use routine diagnostic tools, 48 (53.9 %) document results of routine diagnostic tests, 72 (80.9 %) make interventions on the results but only 37 (41.6 %) document the interventions made. Although all the respondents were aware of the concept of pharmaceutical care (PC), only 55.1 % of them had adequate knowledge of PC, while 93.3% were willing to undergo training to improve their knowledge on PC implementation.
Conclusion: Most community pharmacists routinely use diagnostic tools in Ibadan. However, there is need for improvement on documentation practices.
Introduction
Point-of-care (POC) testing typically involves performing a robust diagnostic test that rapidly produces reliable results outside a laboratory at or near the patient to aid in disease screening, diagnosis, and/or patient monitoring [1-3]. It includes blood glucose testing, blood gas and electrolyte analysis, rapid coagulation testing, rapid diagnosis of cardiac markers, screening of drugs of abuse, urine strips testing, pregnancy tests, faecal occult blood analysis, food pathogen screening, hemoglobin diagnostics, infectious disease testing and cholesterol screening. To improve clinical management (e.g., triage, referral, and treatment decisions), such tests should be convenient and simple to perform, and should have a rapid turnaround of results. With POC testing, the screening or diagnostic processes can be completed during a single clinical encounter, a key difference from laboratory-based testing [4].
POC testing has become established worldwide and finds vital roles in public health [5]. These testing devices have been used in community clinic settings and pharmacies in a number of countries [6]. Its potential operational benefits include more rapid decision making and triage, reduced operating times, reduced emergency room time, reduced number of outpatient clinic visits, reduced emergency admissions and optimal use of professional time. In South Africa, Flobbe et al found out that blood pressure measurement, and tests for serum cholesterol, capillary glucose and pregnancy were the most commonly offered services in pharmacy-based screening programs [12]. Screening tests were conducted less than five times a week, except for blood pressure measurement which was more frequent and less than half of the records kept by respondent pharmacies [12]. The ready availability of these routine diagnostic tools affords community pharmacists the opportunity to perform on-site laboratory services for patients [13]. Moreover, the use of routine diagnostic tools as a part of pharmaceutical care is advantageous because they require small samples and are convenient for patients, portable and allow testing in a variety of locations. For example, hypertensive patients usually check their blood pressure (BP) at community pharmacies [14]. Taking BP measurements in this setting is recommended by some scientific hypertension societies, such as those in Canada [15]. In Nigeria, there are indications that majority of DM patients check their blood glucose status only on the appointment days in the clinic [18]. In this respect, community pharmacists, who are easily accessible to patients, can take up the challenge of doing routine diagnostic tests.
This study was aimed at evaluating the use of routine diagnostic tools among community pharmacists in Ibadan. In addition, it evaluated awareness of the respondents on pharmaceutical care concept as well as the documentation of pharmaceutical care interventions.
Methods
Study setting
The study was carried out in all the 11 local government areas in Ibadan, the capital of Oyo State, Nigeria. With a population of over 3 million, Ibadan is the most populous city in the State, and the third most populous city in Nigeria. Community pharmacists in all the 94 pharmacies registered with the Pharmacists Council of Nigeria (PCN) in the 11 local governments were enlisted for the study. These pharmacies are distributed all around Ibadan city.
Study design
This is a questionnaire-based cross-sectional study which assessed the use of routine diagnostic tools among all community pharmacists in the study location. The questionnaire was divided into two sections. Section A addressed the demographic information as well as basic information on pharmaceutical care (means of awareness, definition, self-rating on the knowledge, level of implementation and willingness to undergo training) while section B addressed the use of routine diagnostic tools, how the skills were acquired, frequency of use, fees charged for the tests and documentation of results. The questionnaire was pre-tested among 5 community pharmacists; the results from the pre-test were not included in the study.
Survey questionnaire was self-administered to the pharmacists in their respective pharmacies. Repeated visits were made for data collection from respondents to the questionnaire.
Data analysis
Data collected were entered into a computer spreadsheet and analysed using descriptive statistics. Categorical variables were compared using Chi-square at a level of significance of p < 0.05.
Results
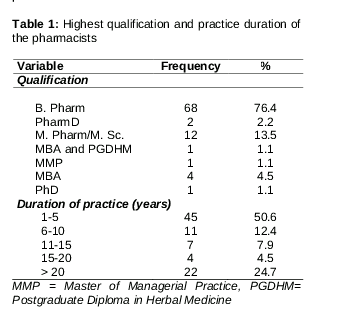
Out of the 94 pharmacists surveyed, the response rate was 94.7%. Most of these respondents (61.8%) were males. The highest qualification and duration of practice as pharmacists are as shown in .
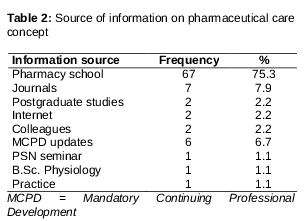
Although all the respondents were aware of pharmaceutical care (PC) concept, 42.7% of them defined PC correctly, 31.5% were partially correct while as many as 23 (25.8%) could not define the concept correctly. Majority of the respondents (49, 55.1%) had adequate knowledge of PC, while 83 (93.3%) were willing to undergo training to improve their knowledge on PC implementation. The rating on the level of implementation of pharmaceutical care concept in the respondents’ pharmacy premises showed that 29 (32.6%) of the participants fully implemented it, 46 (51.7%) implemented it fairly-well, 13 (14.6%) implemented it poorly, while 1 (1.1%) did not implement it. Most of them (75.3%) acquired their knowledge of PC in pharmacy schools ().
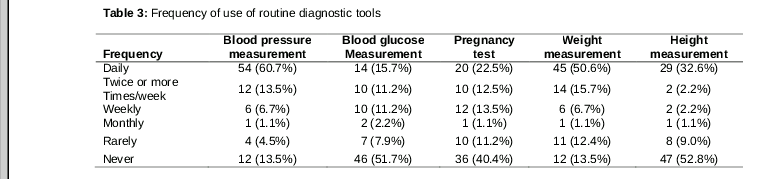
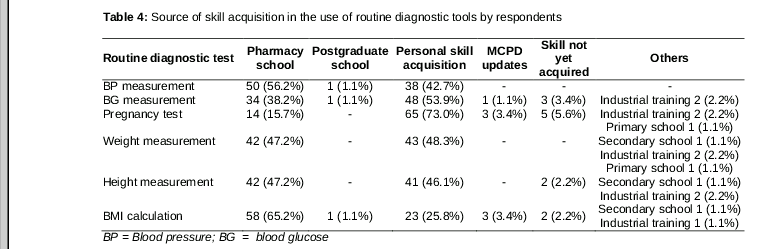
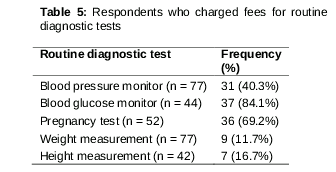
Majority of respondents used routine diagnostic tools in their pharmacies. These tools included blood pressure monitors (87.6%), glucose monitors (46.07%), weight scales (83.1%), and height scales (44.9%). In addition, majority of them (58.4 %) ran pregnancy tests in their pharmacies (). The source of acquisition of skill in routine use of these diagnostic tools is provided in while the proportions of respondents who charged fees for the use of routine diagnostic tools are provided in . While majority of the respondents (80.9 %) reported making interventions following diagnostic tests in their pharmacies, only 41.6 % of them documented such interventions.
Discussion
The study revealed that over 75 % of the respondents used routine diagnostic tools, while only 50 % of these documented their interventions. Although the community pharmacists were aware of PC concept, only 55 % of them had adequate knowledge of the concept.
Generally, the training of a pharmacist in Nigeria does not often include the use of routine diagnostic tools at the level of Bachelor of Pharmacy (B.Pharm.) degree curriculum. With the introduction of the Doctor of Pharmacy (PharmD) programme and developments in pharmacy education, the community pharmacists have acquired knowledge on how to use diagnostic tools. Incorporation of training on the use of these tools is mandatory in existing mandatory continuing education programme for pharmacist. This is vital for increasing the number of pharmacists using these tools as part of their services to patients.
Over 75 % of respondents used blood pressure monitors in this study. This result is similar to an earlier result from a study in Enugu, southeastern Nigeria [22]. As regards service charges for routine diagnostic tests, the blood glucose and pregnancy tests were the tests where most of the respondents charged fees mainly to defray cost of materials used. Although the documentation of intervention in this study is considered poor with even less than one-tenth employing computerized methods, it is comparable to earlier studies in Enugu [22] and Ibadan [23]. Most of those who documented their interventions did so manually. However, our study showed better documentation of interventions when compared with an earlier study in Ghana where 88 % of the pharmacists kept no records of the services they rendered [24].
Conclusion
The findings of this study reveal that a minority of community pharmacists in Ibadan routinely use diagnostic tools in their pharmacies. Moreover, documentation of their related interventions was poor. The need to improve education of pharmacists in provision of basic diagnostic services is vital considering that most patients often consider community pharmacies their first point of call when they are ill.
References
Archives


News Updates